
 A new Guideline for the treatment of cUTI just arrived.[1]
A new Guideline for the treatment of cUTI just arrived.[1]
First, we are glad that this somewhat mundane topic receives the attention it deserves. UTIs are often downplayed as minor infections, but the cUTI variety should not be taken lightly. Many patients still are admitted with life-threatening infections, so prompt recognition and treatment is paramount. The days are gone when almost all infections were caused by pan-susceptible E. coli. Therefore, antibiotic selection is no longer straightforward.
The new Guideline is a 59 page monster. Even without references, it runs 49 pages long, virtually guaranteeing that no one will read the full document. Thankfully, it comes with an abridged Executive Summary which covers the essentials (still running 13 pages long without references). Here are some key points and our take on them.
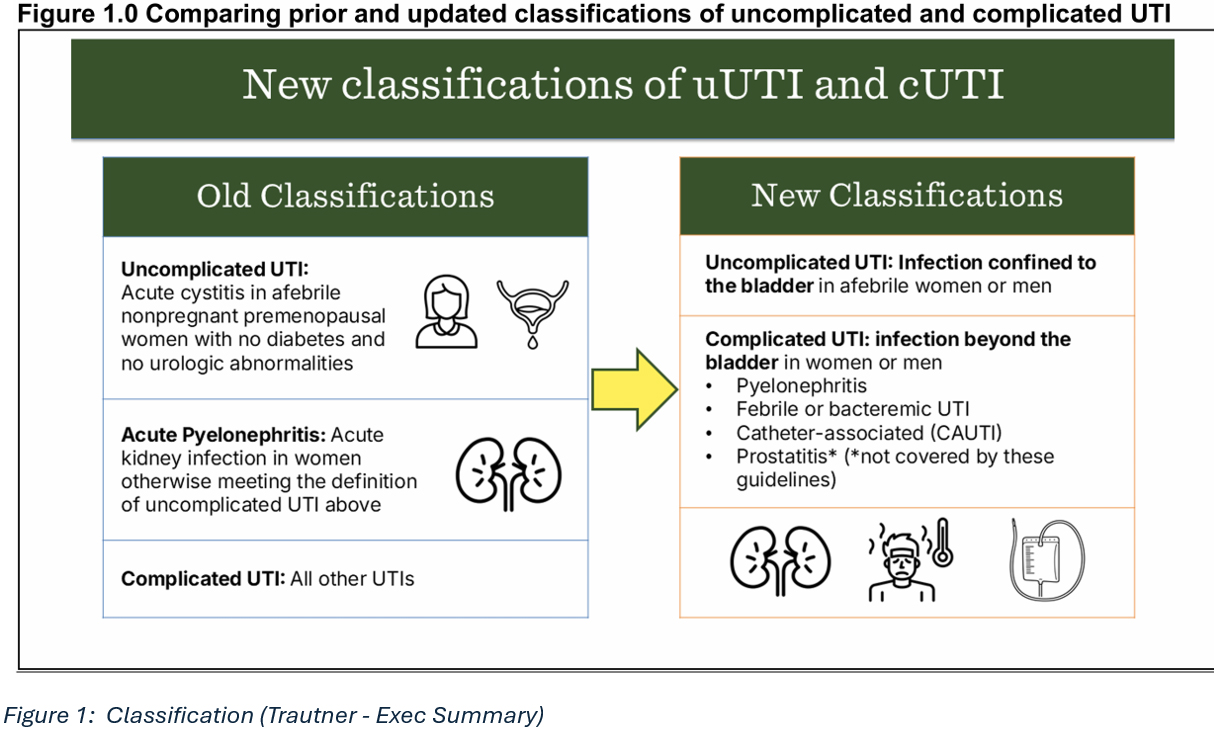
First, gone is the tripartite classification: we are back to the older 2-tiered classification which recognizes uUTI and cUTI, with pyelonephritis now back under the cUTI heading. This makes perfect sense to us and we sincerely hope that the next cUTI Guideline keeps things this way too.
Second, we like the new tiered approach for antibiotic selection based on severity. Assessment should follow a step-wise approach:
(1) severity of illness, OF COURSE, MAKES SENSE
(2) risk factors for resistance, YEP, WE AGREE
(3) patient-specific considerations, SURE THING!
(4) if septic, consider the antibiogram (if local, recent, relevant). Hmm, NOT SO SURE…
Using a recent antibiogram to help with initial empirical antibiotic selection is a recommendation without supporting evidence. The authors acknowledge this by qualifying it as a “conditional recommendation, very low certainty of evidence”. We find this problematic.
Guidelines should be based on hard evidence. This is a higher standard than opinion pieces or ex-cathedra declarations of faith. We feel that (4) has no place in decision making.
Third, we like the lists of antibiotics that are considered appropriate (see below). These were selected based on recent Phase 3 submission trials. While it seems the best source of efficacy data, it creates a dilemma as far as MDR pathogens are concerned.
Registration trials are designed to enroll cUTI cases caused by uropathogens susceptible to BOTH the study drug AND the comparator. This is an FDA stipulation which can be found in all recent protocols. It eliminates from efficacy evaluation those organisms that are not susceptible to both antibiotics, esp. MDR pathogens that are susceptible to the newer test antibiotic but not to the older comparator.
The primary efficacy analysis in FDA pivotal trials analyses is based on the microbiological intent-to-treat (micro-ITT) population (i.e., all patients with a documented bacterial infection). By definition, in this population randomized patients have a baseline bacterial pathogen on culture of urine or blood that causes cUTI against which the investigational drug and control drug have antibacterial activity.[2]
Fourth, we are not happy that antibiotic stewardship considerations feature so prominently in the Guideline. Complicated UTI, regardless of severity, is not uUTI for which stewardship considerations have a major role. The entire ‘stewardship’ concept rings hollow and self-serving when one considers the amount of antibiotic abuse in veterinary medicine. Let’s not forget that cUTIs are not trivial infections, even if mortality is low under the somewhat artificial conditions of clinical trials. Urosepsis and pyonephrosis are very serious conditions that are complications of cUTI one wants to prevent. Actress and Bond girl Tanya Roberts died from fulminant urosepsis and multiorgan failure.

If you made it to Page 30 of the Guideline, you find an interesting section on the Prognostic Impact of Inappropriate Empiric Antibiotic Therapy (IEAT) in cUTI.
We quote:
“an increase in mortality was observed in patients at high risk of mortality with cUTI receiving IEAT, with a pooled adjusted OR of 1.56 (0.99 to 2.46), as compared to patients receiving appropriate empiric antibiotic therapy.”
This suggests a 56% improvement in survival with ‘appropriate’ antibiotic therapy. While this sounds convincing – after all, it confirms our bias that ID docs can make a difference by selecting ‘appropriate’ antibiotics – there are some major caveats: this analysis was based on a meta-analysis of low quality observational studies with all of their inherent shortcomings. No need to say more.
The authors state that using the broadest of coverage in high-risk patients would be defensible to lower mortality; however, they also mention the downside to this approach as it affects antibiotic stewardship and safety / tolerability issues with antibiotic cocktails in order to achieve the most complete coverage (Page 33). We agree, in general, but would also point out that one can exclude gram-positive pathogen coverage like for enterococci right from the get-go. To clarify, there is no need to include vancomycin in any empiric antibiotic combo, if GPCs are absent.
As someone who has stained urine samples during residency, I respectfully disagree with the notion that we need trained microbiologists for this simple task. Good riddance to guidelines that make no use of older diagnostics like Gram stains! This quick and informative bedside test still should have a role, esp. in the context of antibiotic stewardship and UTIs.
 ABBREVIATIONS
ABBREVIATIONS
IEAT inappropriate Empiric Antibiotic Therapy
GPC Gram-positive cocci
MDR multidrug-resistant
micro-ITT microbiological intent-to-treat
REFERENCES
[1] Trautner. Clinical Practice Guideline by Infectious Diseases Society of America (IDSA): 2025 Guideline on Management and Treatment of Complicated Urinary Tract Infections.
[2] Complicated Urinary Tract Infections: Developing Drugs for Treatment. Guidance for Industry. FDA CDER 2018
