

In our last blog we discussed strategic and regulatory issues related to Emblaveo’s clinical development, without commenting much on the REVISIT study results [1].
Today we want to highlight a recurrent problem seen in almost all clinical studies of anti-infectives that no one makes a serious attempt to tackle.
New antibiotics are supposed to be used preferentially against MDR pathogens, not against the majority of infecting bugs which are susceptible to any number of antibiotics. We really would like new antibiotics to be tested in infections caused by a particular MDR pathogen as their ‘claim to fame’ efficacy feature. As it stands, our Phase 3 trials do the opposite: they collect information predominantly on pathogens commonly involved in a given indication, but hardly tell us anything about activity against the rarer problem isolates that we actually would need to learn more about.
Let’s revisit the MDR organism yield of the REVISIT trial. The effort was impressive. This was a multinational trial conducted at 81 centers in 20 countries. Most patients were recruited in China, Turkey, Spain, and the Ukraine; the single participating US center recruited an amazing 21 patients. So far so good.
After 5 (!) years and screening 461 patients with cIAI or nosocomial pneumonia, 422 were actually enrolled. Here is the yield for ‘organisms-of-interest’:
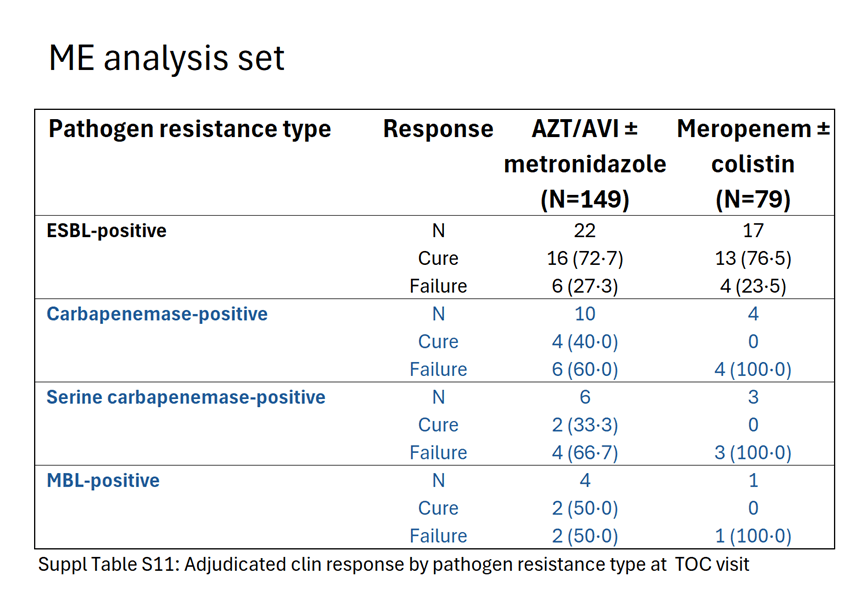
As obvious from the table, the study found hardly any MBL producers, the main reason for existence of Emblaveo. In addition, how should we interpret the data given the extremely small number of microbiologically evaluable cases? Outcome was adjudicated by blinded reviewers, an important quality marker of the study; hence, we can trust their assessment. That said, the rather high percentage of clinical failures in the MBL and carbapenemase-positive subgroups is nothing to be proud of. Again, the numbers are too small to draw any conclusions.
This effort contrasts with the ease with which Falcone et al. were able to prospectively find and enroll MBL patients. At a single center in Pisa they prospectively collected 343 patients with various infections over 3 years.[2]
In an earlier publication, the same group of authors reported on the treatment of MBL bloodstream infections with various regimens. Within 13 months they identified 102 cases of infections caused by MBL producing Enterobacterales prospectively at 3 centers in Italy and Greece.[3]

Remember this next time you visit Tuscany, Pisa, the Torre Pendente and the Piazza dei Miracoli and try not to end up in a local hospital – you’re in an MBL-endemic area.2
Did the REVISIT study at least succeed in showing comparable efficacy to meropenem in cIAI? The answer is a clear and resounding NO. The study was not powered to show NI even if we were to add the 34 cases of cIAI infections from the uncontrolled REJUVENATE trial to the mix.[4]
Let’s get back to MDR pathogen-centered studies. As it stands, clinical trials and guidelines are not really suitable to verify antibiotic activity in any kind of MDR infections. We still enroll based on clinical presentation without knowing anything about the causative organism and its resistance genotype. Our indication-focused registration studies are good at selecting the right patients in a given disease category, like UTI, IAI, skin infection or pneumonia, but agnostic regarding organism species and their all-important resistance-patterns.
In cancer trials we are able to select patients with certain MSI mutations for study. There is sufficient time to do this and other specific testing to preselect patients and assign to treatment. Antimicrobial studies are fundamentally different; sponsors rarely make use of rapid molecular testing to identify organisms of interest and their resistance profiles.
In this age of PCR and genomic testing, the time-honored culture approach should be abandoned whenever possible. We should not have to wait 3 days to obtain culture and susceptibility results, using empiric therapy in the meantime. Rapid diagnostics have come a long way and can provide critical information within hours to select (1) the right antibiotic for our patients, and (2) the right patients for our clinical studies.
We believe Sponsors have a role to play in adapting the newer technologies. Regulators will follow and amend the Guidances and regulatory statutes in light of the ‘new science’.
Rapid PCR based diagnostics are getting cheaper. They are offered as kits by various manufacturers. We are not endorsing any particular product or technology but had a good experience with the bioMerieux BioFire system for identifying CRAB in a recently published trial [5]
Using PCR-based rapid diagnostics makes especially good sense for clinical trials of new antibiotics. This will streamline our enrollment efforts and eliminate the diluting effect of non-contributing pan-susceptible pathogens. Honing in on patients with ‘problem pathogens’, we can then randomize our new antibiotic to existing SOC or BAT. We believe such an approach is vastly preferable to the way clinical trials are mostly done today.
Organism-specific indications have always existed; drugs for malaria and TB, for Helicobacter and C. difficile infections, all have organism-specific labeling. Daptomycin was approved for Staph. aureus bacteremia and right-sided endocarditis. Clearly, these are still exceptions. Truth be told, regulators had a very hard time with the wording of the daptomycin label, as it broke the mold of indication-driven approvals. Nowadays, we have regulatory support for the development of organism-specific antibiotics like P. aeruginosa and A. baumannii.
We’d like to move away from the time-consuming testing sequence (detection of pathogens in specimens – growing them to density for speciation – resistance testing against a panel of antibiotics). This all was fine and good in the days of Robert Koch, but today we should make use of newer technologies not only in hospitals but also when it comes to clinical trials.
ABBREVIATIONS
BAT best alternative therapy
BSI blood-stream infections
CDI Clostridium difficile infection
CPE carbapenem-producing enterobacteriaceae
CRAB carbapenem-resistant Acinetobacter baumannii
ESBL extended-spectrum beta-lactamase
MBL metallo-beta-lactamase
MDR multi-drug resistance
MSI micro-satellite instability
SOC standard of care
REFERENCES
[1] Carmeli Y. Aztreonam–avibactam versus meropenem for the treatment of serious infections caused by Gram-negative bacteria (REVISIT): a descriptive, multinational, open-label, phase 3, randomised trial. Lancet Infect Dis 2025; 25: 218
[2] Falcone M. Clinical Features and Outcomes of Infections Caused by Metallo-β-Lactamase–Producing Enterobacterales: A 3-Year Prospective Study From an Endemic Area. Clin Infect Dis 2024;78:1111
[3] Falcone M. Efficacy of Ceftazidime-avibactam Plus Aztreonam in Patients With Bloodstream Infections Caused by Metallo-β-lactamase–Producing Enterobacterales. Clin Infect Dis 2021; 72:1871
[4] Cornely O. Pharmacokinetics and safety of aztreonam/avibactam for the treatment of complicated intra-abdominal infections in hospitalized adults: results from the REJUVENATE study. J Antimicrob Chemother 2020; 75: 618
[5] Kaye K. Efficacy and safety of sulbactam–durlobactam versus colistin for the treatment of patients with serious infections caused by Acinetobacter baumannii–calcoaceticus complex: a multicentre, randomised, active-controlled, phase 3, non-inferiority clinical trial (ATTACK). Lancet Infect Dis 2023; 9:1072
