

In 2024, the ECDC published a detailed review of flu vaccine studies [1]. In particular, the report examined published trials of newer flu vaccines. As is well known, the older vaccines provide significant protection, but efficacy is diminished in certain populations. Especially the elderly are at an increased risk of influenza due to immunosenescence and have a suboptimal antibody response to vaccination.
The ECDC review was rigorous; studies were classified by quality and checked for bias and other deficiencies. The main emphasis was placed on prevention of laboratory-confirmed influenza and on laboratory-confirmed influenza infections requiring hospitalization. The verdict: Most studies were considered to be of low quality for any efficacy and safety claims. In the words of the ECDC, most studies reviewed provide only “low certainty of evidence”.
Two recent publications in the NEJM had similar shortcomings. Identical in design, GALFLU-2 and DANFLU used a composite endpoint related to hospitalization for primary efficacy assessment. However, for exploratory purposes, they also report the relative vaccine efficacy (rVE) for laboratory-confirmed influenza-related hospitalization which was a key ECDC review criterium.
The term rVE describes the ratio between enhanced and standard vaccine responses. Enhanced stands for improved reactogenicity of the 4x higher vaccine dose tested. Dose escalation is not the only way to further stimulate the immune response; other approaches rely on new and improved adjuvants.
So much for background.
The 2 large Sanofi trials GALFLU-2 and DANFLU compared a 4x higher dose with the standard dose of an inactivated flu vaccine in the elderly (age > 65) [2]. We added this new information to the ECDC’s summary table as follows:
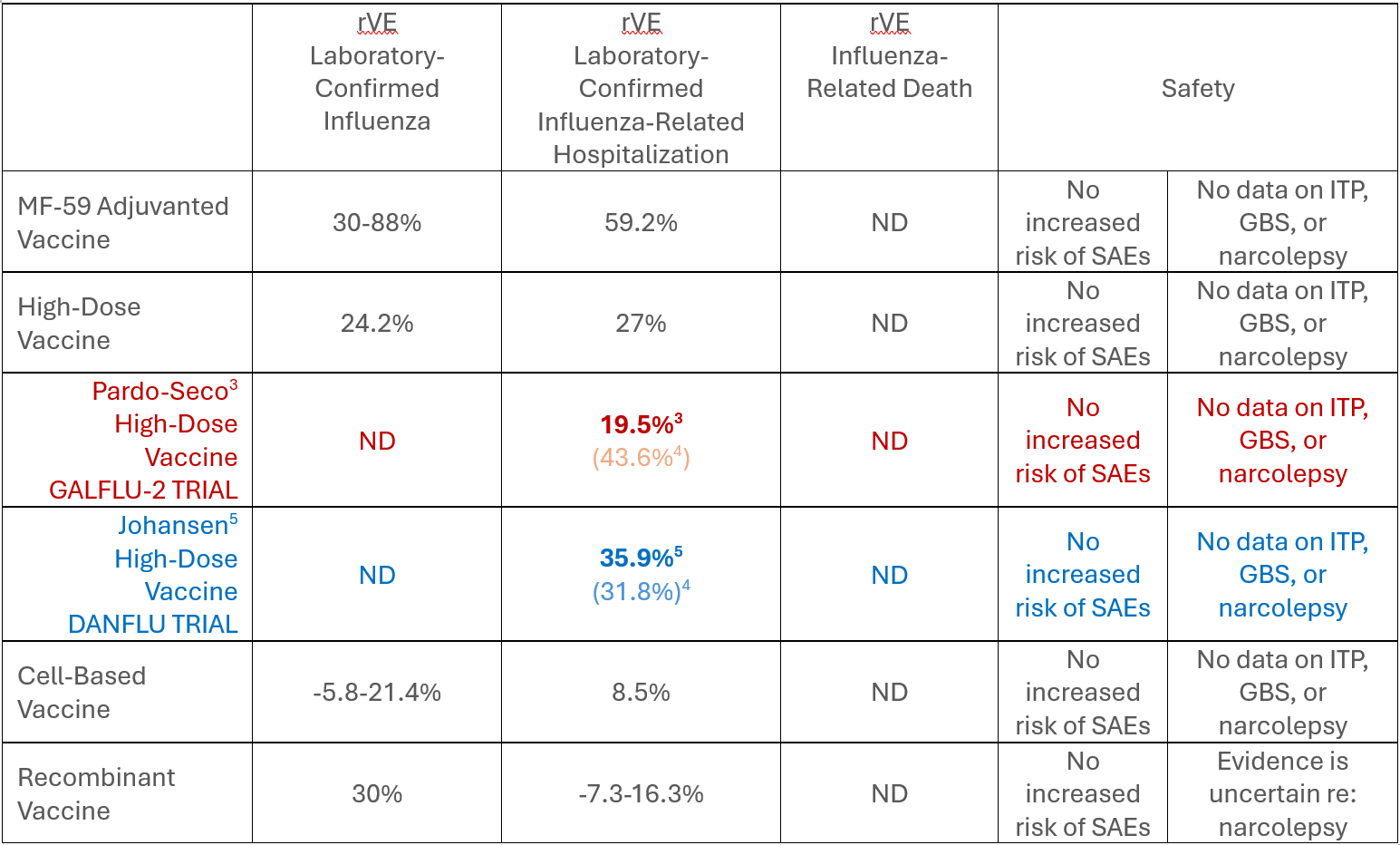
rVE Laboratory-Confirmed Influenza-Related Hospitalization was not the primary endpoint of either trial, but the results were provided and are in the right range. The data suggest improvement in efficacy/effectiveness over standard dosing with the more potent vaccine. Safety, we are told, was on par with the standard-dose regimen. Nonetheless, in the next ECDC review we expect a statement along these lines:
…overall, for high-dose vaccine, certainty of evidence was moderate for the outcome laboratory-confirmed influenza. Certainty was assessed to be low for influenza-related hospitalization (sic!). No assessment was possible for influenza-related death due to lack of data. For serious adverse events, certainty of evidence was low…
However, this would not be a fair characterization of the effort. It is easy to find fault with trials sitting in the ivory tower of an ‘expert reviewer’ coming up with post-fact criticism.
First, how is one to conduct a vaccination study when the incidence of the efficacy endpoint is so rare?
Mind you, we are not trying to show efficacy versus placebo but versus a prophylactic regimen of proven efficacy in the nested subset of elderly individuals and those with death or hospitalization due to documented influenza.
The 2 studies were quite innovative by design. They collected post-vaccination health care data – in huge populations – in separate locations in Europe in a structured way; the role of the company was pretty much hands-off. To execute such trials is a massive effort and deserves praise.[3]
The efficacy results were reassuring; they have meaning for the practicing physician. So much is clear: the higher dose in the enhanced vaccine is certainly not less effective (and actually may be more effective) than the standard dose vaccine. Getting greater certainty would require studies that are just not affordable. They are also not reasonable in the context of a disease with considerable seasonal variability.
Second, how is one to conduct a vaccination study when the incidence of any safety endpoint is so rare?
The published literature mainly speaks of SAEs, the easiest form of AEs to capture. Other more common AEs like fever, malaise, arthralgia, injection site reactions and so on are rarely reported in prospective studies as this requires active monitoring which was not done in the Pardo and Johansen trials.
It would also have been a huge undertaking hardly worth the effort. No doubt, it opens these studies up to critique from those who consider such a design fundamentally flawed. Neither study included long-term follow-up to capture late vaccine sequelae. For example, events that did not make it into the Galicia Hospital Data Base would not be recorded or become known to the investigators. The cut-off for safety data collection was 3 months after vaccination.
Post-vaccination fever may not be particularly concerning, but GBS and other immune reactions may be more worrisome. We are told of 5 SAEs – all in the HD group; there were none in the standard dose arms – that were attributed to the vaccine (1 case each):
- allergic purpura; arthropathy
- COPD exacerbation and acute infection
- acute bronchospasm w/respiratory failure and hypoxia
- anti-synthetase syndrome
- pericarditis
Clearly, these are all immune-related SAEs, and we are left to wonder whether there could have been more had there been a longer observation period for AEs. In other words, was the low AE/SAE incidence a consequence, an artifact of study design? This fishing net had some big holes, it seems.
In conclusion, these were hands-off mega-trials, with finely adjusted tools to measure vaccine effectiveness and rather crude tools to capture safety issues. Safety was not neglected: we are glad that the GALFLU-2 study at least was run under the auspices of Santiago de Compostela, the patron saint of enhanced flu vaccine recipients.
All is good.
ABBREVIATIONS
GBS Guillain-Barre syndrome
ECDC European Centers for Disease Control
rVE relative vaccine effectiveness
SAE serious adverse event
REFERENCES
[1] European Centre for Disease Prevention and Control. Systematic review update on the efficacy, effectiveness and safety of newer and enhanced seasonal influenza vaccines for the prevention of laboratory confirmed influenza in individuals aged 18 years and over. Stockholm: ECDC; 2024
[2] GALFLU-2: quadrivalent high-dose inactivated influenza vaccine (Efluelda, Sanofi) OR quadrivalent standard-dose inactivated influenza vaccine (Influvac Tetra, Viatris); DANFLU: quadrivalent high-dose vaccine (Fluzone High-Dose Quadrivalent/Efluelda/Efluelda Tetra, Sanofi) OR the quadrivalent standard-dose vaccine (VaxigripTetra, Sanofi)
[3] Pardo-Seco J. High-Dose Influenza Vaccine to Reduce Hospitalizations. NEJM 2025;393:2303
[4] rVE values as quoted by Neuzil editorial
[5] Johansen N. High-Dose Influenza Vaccine Effectiveness against Hospitalization in Older Adults. NEJM 2025;393:2291
[6] Neuzil K. Current and Emerging Approaches to Evaluating Influenza Vaccine Performance. NEJM 393; 23: 2361

