

The pivotal ConfIdeS study has finished enrollment and is now with the FDA. IdeS is imlifidase, with the brand name Idefirix. It has been conditionally approved by EMA and is on the market in Europe since 2020.
Idefirix is a niche product, an orphan drug. It is a cysteine protease that cleaves IgGs of all classes, and it does so very effectively and quickly. It destroys IgG autoantibodies within a few hours. These antibodies would otherwise prevent organ transplantation for recipients who became highly sensitized to HLA antigens due to prior pregnancies, transfusions or transplantation. In other words, it makes transplantation of organs possible without the risk of a hyperacute rejection, even in patients with incredibly high cPRA scores which is an indicator of crossmatch incompatibility.
The US ConfideS study enrolled patients who are highly sensitized, those with a cPRA ≥99.9%. ‘Highly sensitized’ is a misnomer in this case: this entry criterium is so strict that it selects only for super-ultra hyper-extra sensitized patients.
It took Hansa approx. 2 ½ years to enroll 64 patients in the ConfIdeS study
Finding such patients must have been incredibly difficult. For them, transplantation is a race against the clock. Timely desensitization is nearly impossible. Existing desensitization programs based on plasma exchange just don’t work nearly as well and as fast as idefirix and right now there is no alternative Therefore, a true control arm does not exist. That’s why the ConfideS protocol reads more like an artificial construct. It makes all kinds of allowances for an alternative treatment for hypersensitized patients when there is no idefirix-like agent available.
Seven years after the EMA, FDA will get to review the pivotal Phase 3 ConfIdeS trial, plus an assortment of other study data which represent the uncontrolled experience with Idefirix
While our last blog dealt with FDA ‘flexibility’, this blog is all about FDA response to a novel break-through therapeutic. Of course, it might be a lot easier for the Agency to review and approve yet another run-of-the mill PD-1 or JAK inhibitor.
There is a reason why the enthusiasm for idefirix is a bit subdued. Idefirix is not a panacea for the niche it is addressing, the highly sensitized ESRD patients. Elimination of IgGs is temporary and rather short-lived, just long enough to allow transplantation and provide protection of the organ in the immediate post-transplant period. As the drug effect wears off, IgGs return and so do specific autoantibodies against DSA and anti-drug antibodies (ADA). Given the half-life for IgG of approx. 21 days, humoral immunity will fully return within 1-2 months after transplant. And here lies the problem.
Ideally, one would like to dose idefirix repeatedly titrating its effect over a longer time post-transplant, like other desensitization protocols for CMI suppression. Regrettably, idefirix is a foreign protein and highly immunogenic. There is a significant risk of an anamnestic response on repeat dosing, even with premedication. AMR occurs rather early, in 28% of patients within 1 month of transplant[1].
It seems that idefirix cannot be made less immunogenic. We don’t know whether Hansa pursued other ways of reducing ADA as has been done for uricase inhibitors, using a PEGylation approach or co-administration / premedication with methotrexate or sirolimus as done with pegloticase, a treatment for hyperuricemia.
Still, in the absence of a better drug, idefirix is a game changer. There is really no drug in sight that could compete with idefirix making transplantation possible.
EMA recognized that dilemma and approved it in Europe for patients who are not candidates for transplant with a very high cPRA score which makes finding a suitable donor next to impossible. EMA felt that the benefits for these patients outweigh the risks.
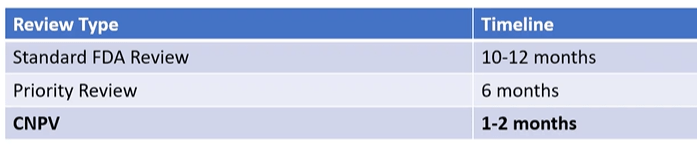
As mentioned earlier, the company has now submitted its dossier to the FDA, and a PDUFA date was set for Nov 2026. This amounts to a 10-month standard review. Why so late? Like Hansa, we would have expected 6-month Priority review given the unmet medical need. After all, idefirix is a BTD drug for a very small group of patients who have run out of options. The ConfIdeS Phase 3 study was conducted at 25 US transplant centers; the list of investigators reads like the Who-Is-Who of kidney transplant gurus. It should have met FDA expectations and led to fast-tracking.
We know the Agency has all kinds of ways to accelerate reviews. In this case the data package is relatively small, a single Phase 3 pivotal trial. Hence, this should not be a colossal task for a Medical Reviewer.
We hope that FDA and the company explore options like conditional approval and faster review as is now possible in select cases. The CNPV program comes to mind which is still a pilot. See table below for review timelines.
Hansa is developing an improved version of idefirix. HNSA-5487, another biological, has already finished Phase 1 testing reportedly with good results (NICE-1 trial) . However, information is still scant as publications are missing. Our information is solely based on Hansa press releases.
HNSA-5487 has a fast onset of action just like idefirix, but the suppression of S-IgG by >75% still only lasts for ~10 days. Development of ADAs seems less of an issue, making repeat dosing potentially feasible. We have to take their word for it, but this would be a substantial improvement.

Surprisingly, HNSA-5487 is not being developed for the idefirix indication (ie, enabling transplant in the highly sensitized) but for neurologic autoimmune diseases like gMG and NMO. In these indications it has to compete against FcRn inhibitors and other biologicals already on the market.
FcRn inhibitors have a MoA quite different from idefirix: They decrease the recycling of IgGs including autoantibodies. However, onset of action is rather slow and IgG levels only drop by approx. 55-65% at best. Thus, IgG lowering is insufficient given the short time window available for transplantation (Fig. 2). However, in combination and as a follow-up to idefirix they could be used, at least conceptually.

Several mAbs are routinely used after transplant and all need dose-adjustment when co-administered with idefirix, HNSA-5487 or an FcRn inhibitor. Such polypharmacy becomes complicated; it requires orchestration by a dedicated team of experts at specialized centers. We trust it can be done!
ABBREVIATIONS
ADA anti-drug antibody
AMR antibody-mediated rejection
BTD breakthrough designation
CNPV Commissioner's National Priority Voucher
cPRA calculated panel reactive antibodies
DSA donor specific antibodies
ESRD end-stage renal disease
FcRn Fc receptor neonatal
gMG generalized myasthenia gravis
MOGAD Myelin Oligodendrocyte Glycoprotein Antibody Disease
NMO neuromyelitis optica
PDUFA Prescription Drug User Fee
PUBLICATIONS
[1] Kjellman C. Outcomes at 3 years posttransplant in imlifidase-desensitized kidney transplant patients. Am J Transplantation 21: 3907, 2021
[2] Tulstrup S. HNSA-5487 demonstrates very rapid and highly robust IgG reduction and clear redosing potential in Phase 1 FIH trial. 20241007_HNSA-5487_12MonthAnalysis_Presentation.pdf
Hansa PR March 3, 2026. PDUFA Action Date for Hansa Biopharma’s Imlifidase BLA Set for December 19, 2026 | Hansa Biopharma (accessed 3/22/2026)
