

Just imagine you were tasked to conduct a seasonal flu study in household contacts of a symptomatic index case. Your intervention may be (your choice): pre-season vaccination, pre-exposure prophylaxis, or some non-anti-infective protective measure such as wearing a face mask, taking a vitamin or analgesic that is believed to confer benefit.
Of course, your study would be a placebo-controlled trial. Not only because the FDA demands it, but also because a superiority study avoids a much larger NI trial. Even so, the size of your prophylaxis study would be quite large, because the event of interest is rare. A placebo arm is defendable as ‘bad outcomes’ are infrequent and manageable.
Our innate immune system is well equipped to deal with viral respiratory infections. Exceptions exist, but the common cold is usually self-limited and trivial. Hence, in order to prove that your intervention can be effective, you would want to find patients that are neither too sick nor too healthy. If too sick, they would not qualify for a placebo trial; if too healthy, the trial would miss a possible benefit and end up giving a false-negative result.
Let’s agree on this premise: The benefit of prophylaxis needs to be shown in some concrete and patient-relevant way. Death is unlikely to be a discriminating feature in a flu trial, but hospitalization, prevention of complications or worsening of symptoms would seem useful as efficacy parameters. It really boils down to demonstrating a clinically relevant benefit.
SARS Covid-19 has changed a lot since the start of the pandemic.[1] Covid-19 behaves just like another common cold virus without the complications and mortality seen originally. Like the flu, it is more a nuisance than the big scare of former years. This makes the design of a PEP study tricky.
Ideally, you’d like to study an ambulatory group of recently exposed individuals with significant risk factors for complications, those who cannot tolerate even trivial respiratory infections too well. PEP study candidates would have some chronic disease with mildly impaired immunity (elderly, COPD, smokers, CVD, DM, steroids, obesity); you certainly don’t want to enroll healthy adolescents. Practically speaking, you would focus on an elderly population with multiple risk factors.
Too many Covid studies failed recently because sponsors ignored the impact of vaccines. [1]
Companies are well advised to enroll only anti-vaxxers for trials of the next Paxlovid!
So, if you did a Covid-19 treatment trial with an antiviral in a mainly healthy, mainly mid-aged adult population without major risk factors for bad outcomes, what kind of outcome could one reasonably expect? With early treatment of Covid-19 infected patients, ensitrelvir delivered a Tamiflu-size benefit: a shortening of symptoms by 1 day.
Likewise, with ensitrelvir for PEP, we would predict some small protective effects, ie, a lower rate of infection, a shorter duration of viral shedding, reduction in VL, lessening of signs and symptoms related to the RTI , and faster improvement. We would predict all of the above as a trend, not necessarily with a P-value < 0.05 – assuming drug PK in the therapeutic range.
Indeed, such was the case with the SCORPIO-PEP ensitrelvir study.[2] The drug showed a lower incidence of “Covid-19 infections” (2.9% vs 9%) in the primary efficacy analysis.
Let’s look at some definitions more closely. “Covid-19 infection” was defined as:
- Covid-19 PCR conversion to positive
PLUS - presence of ≥1 “Covid-19 symptom” during a 10-day observation period (see the list below):

Except perhaps for taste and smell perversion, these are non-specific respiratory infection symptoms. We would argue that these are inconsequential and totally irrelevant for most patients. They may be caused by adenovirus, parainfluenza, or a hundred other viruses to which we are regularly exposed. Attributing reduction in soft criteria to ensitrelvir puts it on the level of acetaminophen: Tylenol could have done just as well.
Let’s face it: SCORPIO-PEP is a strange trial by design. It was well suited to detect treatment effects of a trivial nature:
- only 37% of study participants had what the authors called ‘risk factors for ‘severe illness’. As nobody enrolled required hospitalization, the ‘severe illness’ moniker is plain wrong.
- patients older than 65 yrs made up only 9% of the enrolled population
- the average age of household contacts receiving prophylaxis was 47 years.
Here are the key results:
- The incidence of ‘Covid infection’ (as defined above) was
9% on placebo, and 2.9% in the ensitrelvir arm, a statistically significant difference of 6% - In other words, the number needed to treat (NNT) is ~17
- No safety issues
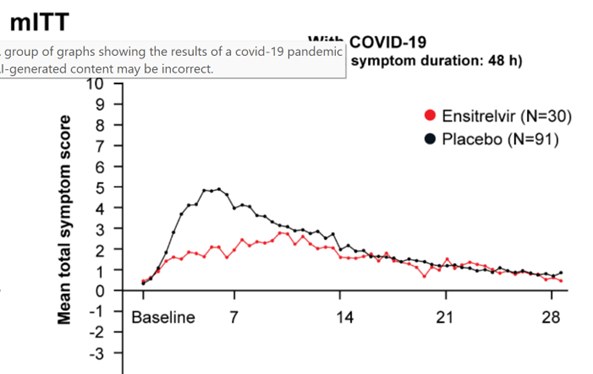
The authors state that symptoms in those who contracted Covid were less pronounced in the ensitrelvir group; a graph below shows us a 2-3 point delta ‘bubble’ in the first treatment week (Fig.1). In light of the large range of the symptom score (0-to 40), this reduction looks rather pathetic.
Even ensitrelvir’s antiviral impact was unimpressive (Fig. 2):
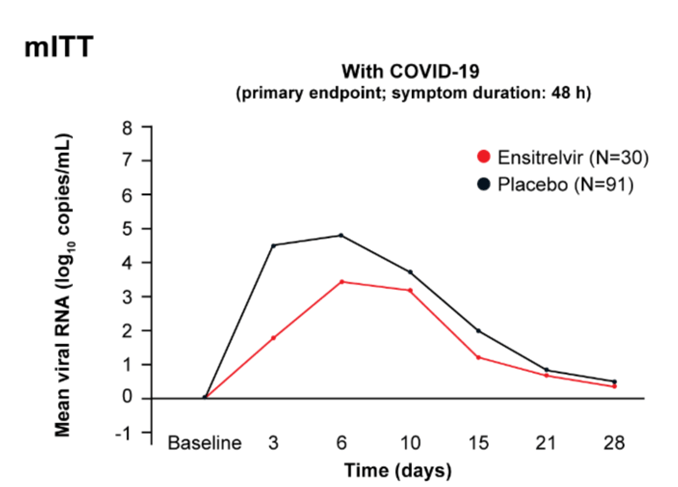
Okay. So far, so good.
If PEP with ensitrelvir reduces the number of days of cough, fever, malaise or anhedonia only slightly, it is not going to make a big splash in the market, right? WRONG.
Remember Tamiflu? Oseltamivir reduced flu symptoms by approx. 1 day, if treatment was started early (within 24 hours). That may not seem like much of a benefit by most people’s standards, but the drug still generates approx. $300 mio in yearly sales during non-pandemic times. Paxlovid sales in 2025 were still above $1 bio despite decreasing performance, high pill burden and a long list of DDI related to ritonavir.
Actually, there is a lot to like about ensitrelvir. Compared to the pill burden of Paxlovid, ensitrelvir is a once-a-day drug. This makes dosing easier for the patient, and COGs lower for Shionogi. It is unencumbered by the ritonavir DDI.
In conclusion, a large PEP study of ensitrelvir showed small benefits. The authors point out that these results are better than for Paxlovid or molnupiravir, but they are not stellar. We believe efficacy may be of the same order as wearing a loose-fitting face mask.
What comes next? Shionogi, a company based in Osaka, has a long and successful history developing anti-infectives. Ensitrelvir is already approved in Japan for Covid-PEP based on this study. In the absence of a demonstrable clinical benefit, approval in the US and EU may get some serious push-back from the FDA, and even more so from payors. Shionogi will have to justify its label and pricing. This may be difficult for HHC < 65 years of age.
We know of no example where an efficacious drug would not also work for prophylaxis. With a short 5-day course, safety is not much of a concern, but pricing is.
ABBREVIATIONS
COGs cost of goods
COPD chronic obstructive pulmonary disease
CVD cardiovascular disease
DDI drug-drug interactions
DM diabeter mellitus
HHC house-hold contacts
NI non-inferiority
NNT number needed to treat
PEP post-exposure prophylaxis
REFERENCES
[1] Butler C. Oral Nirmatrelvir–Ritonavir for Covid-19 in Higher-Risk Outpatients. NEJM 2026;394:1583
[2] Hayden F. Ensitrelvir for Covid-19 Postexposure Prophylaxis in Household Contacts. NEJM 2026, 394:190
