

Quick: What do you associate with the abbreviation ‘TCR’? Does your immunology-trained mind automatically default to ‘T-cell receptor’? Or is your first guess ‘Tissue Cross Reactivity? Our neural networks can deal with ambivalence and will make the right associations, eventually. Language is imprecise by design and allows for wobble.
Things become really confusing when authors refer to “TCR cross-reactivity”. Again, neural networks to the rescue – we implicitly understand what’s meant.
This blog is about TCR = tissue cross reactivity. The term relates to the fact that antibodies sometimes lack precision targeting a certain receptor. In some cases, there is a variable amount of give, a certain degeneracy, a bit of promiscuity. A lack of singularity, if you will.
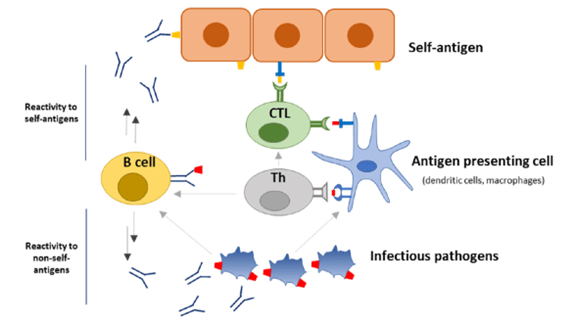
Figure 1: From: Trier N. Ref. [1]
A recent article by Dai et al. makes for interesting reading.[2] It describes a rapid technique to characterize the binding of a large number of mAbs in clinical development or approved (N=174, to be exact) to over 6,000 (!) extracellular proteins. They found cross-reactivity (or off-target binding) with 28% of them.
Author Aaron Ring and the Adimab team are immunology experts with deep understanding of mAb technology. They know all about mAb specificity and/or lack thereof, often called polyreactivity or polyspecificity. This observed high frequency of off-target engagement came probably as a surprise; the article concludes with the recommendation to test for target promiscuity early in drug development.
Immunology is the science of the body’s ability to distinguish self from non-self, the recognition of minute differences in tissue properties, the ability to respond to new antigenic markers presented by invading microorganisms or the neoantigens released at times of tissue injury (think DRESS syndrome). The positive and negative selection process of T-cells is a marvelous process that seems to work extremely well, decreasing the odds of developing an autoimmune disease during lifetime. Our B- and T-cell reservoirs have developed a sophisticated defense system which is both highly conserved and highly specific while being flexible enough to respond to almost any foreign signal.
TCR testing is already part of the routine preclinical testing process required by Regulators worldwide. Off-target toxicity or lack of selectivity rarely rises to a level of clinical concern with mAbs, the predominant class of biologicals. This is quite remarkable: mAbs are considered much safer than NCEs, partly because of their pin-point efficacy. This property of antibody B-cells maturation and antibody specificity is quite amazing, and the same holds true for mAbs produced in ex-vivo in bioreactors. Hence, we take target specificity as a given and are mainly concerned about ADAs. Indeed, package inserts for biologicals do not even mention TCR test results.
This is for good reasons. TCR testing in-vitro on human tissues is problematic as non-specific binding may be misleading. Therefore, preclinical TCR testing is considered a screening test, with caveats attached. It may predict a problem for development but should be seen as just one piece of a jigsaw puzzle, in need of confirmation, to be evaluated in context with other findings. At least that was the opinion of a Consortium of Experts from industry, published in 2010.[3] However, time does not stand still, and much has been learned since then.
Cunningham et al. provided a list of examples from mAb development when cross-reactivity was clinically relevant. While changes to the PK profile can be dealt with, more concerning is off-target toxicity.[4] The authors make the point that testing procedures for cross-reactivity are incomplete and lack standardization. In their words, a “deep, systematic study of antibody specificity is lacking”.
A slightly different view is presented by Trier et al.[1] The authors feel that antigenic mimicry is not the underlying cause of many autoimmune diseases. They make the point that many times cross-reactive antibodies are clinically silent and do not contribute to the development of autoimmune diseases.
Are we too complacent when results turn positive on TCR testing? Should the Dai study make us rethink our approach to TCR testing? What exactly should one do with a positive finding on high-sensitivity TCR testing? There is no threshold or cut-off as to when to call a signal relevant. The more sensitive the methodology, the more cross-reactivity is to be expected.
This situation reminds us of the early days of PCR testing for Legionella on bronchial samples. Just about every test came back positive, while culture and antigen tests remained negative. Hardly anyone had Legionellosis and required specific treatment. Clearly, an overly sensitive test resulted in large numbers of false-positive results.
There are no easy answers here. More testing is not always helpful, if we don’t know what to do with the results. As long as we cannot even interpret the results of existing test protocols, having a more sensitive method is unlikely to eliminate ambiguity.
Therefore, our approach to TCR testing has not changed.
Since the Consortium published its recommendations in 2010, almost 2 decades of biological research have gone by. This fact alone should justify a renewed look at current TCR practices as the field is so dynamic.
ABBREVIATIONS NCE new chemical entity TCR T-cell receptor TCR Tissue cross-reactivity DRESS Drug Reaction with Eosinophilia and Systemic Symptoms ADA antidrug antibody REFERENCES [1] Trier N. Antibody Cross-Reactivity in Auto-Immune Diseases. Int. J. Mol. Sci. 2023, 24, 13609 [2] Dai Y. Off-target reactivity in clinical monoclonal antibodies, Structure 34:1; 2026 [3] Leach M. Use of Tissue Cross-reactivity Studies in the Development of Antibody-based iopharmaceuticals: History, Experience, Methodology, and Future Directions. Toxicologic Pathology, 38: 1138-1166 [4] Cunningham O. Polyreactivity and polyspecificity in therapeutic antibody development: risk factors for failure in preclinical and clinical development campaigns. mAbs, 13:1, 1999195
