

There are MDR pathogens, and there is carbapenem-resistant A. baumannii, aka CRAB.
This surely must be one of the most formidable bacterial organisms. It has resistance mechanisms second to none. When found in patients, it is very difficult to eradicate and extremely difficult to get rid off, once established in hospitals. So far in the US, we rarely have to deal with carbapenem-resistant organisms; CRAB is more prevalent in some European countries such as Spain, Italy, and Turkey. Southeast Asia probably has the highest prevalence and incidence of CRAB patients. Intensivists likely have to deal with this pathogen; it is often the last organism standing after several rounds of antibiotic therapy.
Hospitals are not proud admitting they have an ‘Acinetobacter problem’, which leads us to believe that infections are greatly underreported. We have heard from ICUs in the Middle East that had to deal with CRAB infections routinely, mostly unreported.

No article on CRAB should omit a reference to the ordeal Dr. Thomas Patterson had to go through. He acquired a life-threatening CRAB infection as a tourist in Egypt. The book, written by his wife, is highly recommended for anyone who wants to learn more about CRAB, its virulence and the challenges clinicians and patients face.[1] An investigational cocktail of phages finally controlled his infection, which did not respond to any existing antibacterials. We agree with the book reviews below: a medical thriller.
| “A memoir that reads like a thriller” New York Times Book Review “A fascinating and terrifying peek into the devastating outcomes of antibiotic misuse-and what happens when standard health care falls short” Scientific American |
Cascio et al. wrote an up-to-date article on CRAB therapies.[2]


The authors provide an excellent review of literature, a messy task as most ‘studies’ are retrospective and uncontrolled. Reviewers have to deal with case series, combination therapies, and methodological problems. Most of hese anecdotal ‘studies’ are low quality publications that take up an inordinate amount of space in most reviews, disproportionate to their value.
In situations like this, it becomes difficult to separate fluff from the few hard facts we have. All too often the PK/PD properties of the drugs we use for CRAB infections are ignored. Mind you, we are talking about CRAB, not the carbapenem-susceptible acinetobacters for which treatment is easier. Likewise, we are focusing on severe CRAB infections, like HAP/VAP and bacteremia, not skin infections or UTIs.
Bottom line: One cannot rely on tigecycline or the polymyxins for severe respiratory CRAB infections.
Tigecycline is still being used, mainly because clinicians only look at its in-vitro activity against CRAB which is misleading. Intensivists like to use the drug off-label at high IV doses (100 mg IV q12h) for HAP/VAP as it is well tolerated, thinking that ‘more is better’. However, there is absolutely no evidence higher doses improve outcomes. Several pharmacologists have pointed out that higher doses do not increase levels of free tigecycline, a rare paradoxical effect.
Tigecycline is bacteriostatic, not bactericidal and has poor lung and ELF penetration. Tigecycline is a drug with a low free (unbound) fraction; free AUC is the PK determinant of efficacy. This makes a direct application of MIC data to the clinical situation problematic; it is the probable reason of the failure of several tigecycline trials for pneumonia.
Pfizer has never conducted prospective clinical studies with tigecycline in acinetobacter infections, let alone CRAB. Therefore, the clinical practice of using low- or high-dose tigecycline is hard to defend.
| Cascio et al. do not recommend tigecycline for any serious CRAB infection, pulmonary or otherwise |
Polymyxin / Colistin are drugs with exceptionally low MICs for all acinetobacters, including CRAB. As such they have become the ‘go-to agents’ for serious infections, despite the recognized toxicity, mainly related to dose and treatment duration. Mandell’s textbook has a lengthy section on both drugs, with much ink spilled over the rather confusing dosing recommendations [3], [4]. The authors pointedly state that a therapeutic level can only be achieved in the presence of reduced GFR. In other words: these drugs are underdosed out of concern for nephrotoxicity, an inevitable side effect with more prolonged therapy. On top of this, they have poor lung penetration. Taken together, the drug levels of polymyxin / colistin are likely subtherapeutic if prescribed according to label.
Since their entry into clinical use in the mid-60s, they have not been studied thoroughly, as newer and less toxic antibiotics have replaced them.
| Cascio et al. state that polymyxin / colistin is NOT appropriate for pneumonia caused by CRAB infection |
We also agree and support the other “CLINICS CARE POINTS” at the end of the Cascio article regarding the use of cefiderocol and SUL/DUR.
The following are some additional thoughts from our vantage point:
- Work on acinetobacter-specific phage therapies is underway; we hope this leads to the next big therapeutic advance
- The availability of rapid PCR-based diagnostics is important for early detection and monitoring in critically ill patients
- We are not sure whether TDM has a role for cefiderocol or any other drug; there is simply not enough data
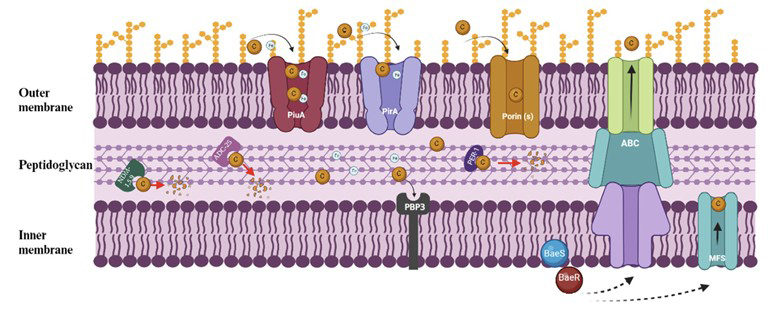
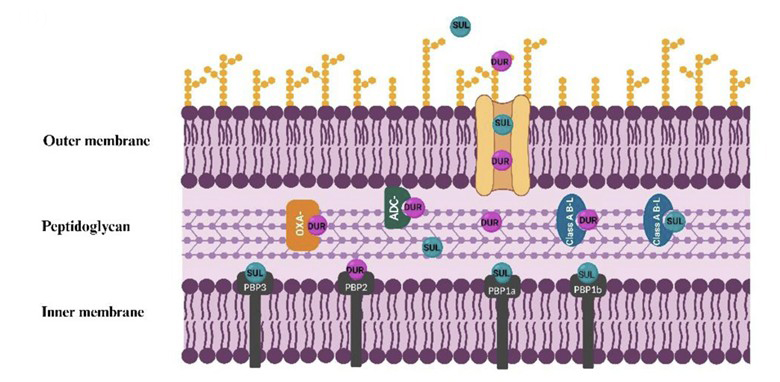
- Emergence of resistance to cefiderocol and SUL/DUR is a given. It will happen probably faster with Acinetobacter than with most other bacteria. We’d love to be proven wrong on this account, but increased use of these 2 new agents will drive resistance. FYI, the article by Karruli et al. provides an excellent review of molecular resistance mechanisms of both compounds and is recommended reading [5] .
Prospective well-controlled studies for CRAB are extremely difficult to conduct; we expect that future publications will give us more ‘real world’ data and meta-analyses. The Cascio paper is a solid attempt to make sense of the low quality of existing data sorting out fact from fiction and extracting the few hard facts from a sea of crappy CRAB articles.
For these efforts we are grateful.
ABBREVIATIONS
AUC area under the PK curve
ELF epithelial lining fluid
HAP hospital-acquired pneumonia
HD high dose
HSA human serum albumin
TDM therapeutic drug monitoring
VAP ventilator-associated pneumonia
REFERENCES
[1] The Perfect Predator: A Scientist’s Race to Save Her Husband from a Deadly Superbug: A Memoir. Strathdee S, Patterson T.
[2] Cascio A. How to Treat Carbapenem Resistant Acinetobacter baumannii Infections: Current Knowledge and Personal Viewpoints. Infect Dis Clin N Am 40 (2026): 23
[3] Pogue J. Polymyxins (Polymyxin B and Colistin), Chapter 31. Mandell’s PPID 10th edition 2025, Elsevier
[4] Nation R. Colistin: How should it be dosed for the critically ill? ASID Gram Negative Superbugs Meeting. Gold Coast. Presentation slides. 2 – 3 August 2013
[5] Karruli A. Cefiderocol and Sulbactam-Durlobactam against Carbapenem-Resistant Acinetobacter baumannii. Antibiotics 2023, 12, 1729
For an up-to-date review of CRAB epidemiology, treatment options and pipeline:
Makwana N. Global strategies to fight carbapenem-resistant Acinetobacter baumannii (CRAB) infections. Microbial Pathogen 214, 2026, 108412
The novel phages depicted in the banner are taken from:
Chen X. Isolation and characterization of two novel phages with lytic activity against multidrug-resistant Acinetobacter baumannii strains: potential for phage therapy. Nature Portfolio Scientific Reports (2025) 15:43520
