
Searching data on antibiotic use in surgery prophylaxis, I came across an article from the Mayo Clinic [1]. The authors mention that approx. 75% of patients that developed surgical site infections did not get proper antibiotic prophylaxis. Errors were made in (1) selection of the antibiotic, (2) timing of administration, (3) antibiotic dosing, or (4) lack of repeat dosing when a short half-life drug would have required a second dose during surgery.
This was a retrospective review and these performance criteria were applied quite strictly. For instance, an error related to re-dosing could be 3-fold: not done when required; done but with a wrong dose, or done but not at the right time.
This all makes sense but I am not sure I would have gotten all these details right myself, even come close. Actually, I would have done very poorly because I did not know that aminoglycosides are supposed to be dosed according to ideal body weight (IBW).
So, what is ideal BW? Thankfully, Columbia University [2] provides the answer:
IBW (males) = 50 kg + (2.3 x height in inches > 60 inches) [3].
Can a formula be correct which mixes kg and inches, metric and imperial units? Well, you may have to convert your patient’s weight from pounds to kg first but that’s straightforward if not easy to remember: 50 kg is equivalent to 110.231 lbs.
Now we are making progress: let’s assume our patient weighs 68 kg (149.914 lbs) and is 170 cm tall (66.9291”). With 7 inches over 60 inches, we get an IBW of 66.1 kg. Assuming our anesthesiologist does not have to make adjustments for: severe illness, obesity, female gender, renal compromise, or loading dose, we can now order gentamicin or tobramycin confidently at 2 mg/kg IBW q8h IV, or 132 mg per dose, rounded off to 130 mg/dose. If you prefer a 1.5 mg/kg IBW q8h regimen, you end up with a dose of 100 mg.
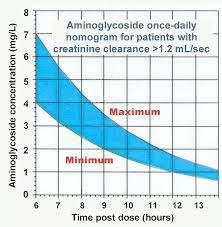
Note: Dosing for high-dose once-daily kidney-sparing extended-interval regimens has its own formula and PK profile (see Fig. 1). Dosing for Gram-positive synergy, for mycobacterial infections, and pediatric infections is different as well, of course. And for patients weighing less than IBW, one should use actual BW (ABW), for those with BW >20% above IBW (or is it: > 30%?), you should use DBW (which stands for “Dosing Body Weight”).
Obviously, these dosing guidelines require several megabytes of storage on your computer, and the equivalent of approx. 50% of my cerebral memory banks. However, it is important to heed these dosing recommendations in order to avoid aminoglycoside-associated nephro-, neuro-, and ototoxicity, and a later court summons. Hence, we should also look into proper infusion times and when to measure peak and trough levels.
The package insert specifies a 30-60 min infusion time for our 130 mg dose; peak measurements after 4 half-lives should be done 30 min post-infusion. The goal is to have a peak-to-MIC ratio of approx. 10 for efficacy. Okay, now let’s move on to vancomycin, the other major drug used in surgical prophylaxis.
For starters, vancomycin is dosed according to actual body weight (ABW). No need to calculate the IBW but conversion of BW into kg is still needed (for estimating creatinine clearance with the Cockcroft Gault method). In hospitals using the metric system, conversion of S-creatinine (1 mg/dL = 88.4 µmol/L or 1 µmol/L = 0.0113 mg/dL) to the old units is also required.
At the recommended dose of 12-15 mg/kg, our 68 kg patient should receive a maintenance dose between 816 – 1020 mg IV q12h, with a loading dose possibly as high as 1500 mg. These doses would be infused over 60 min. We no longer check peak concentrations as they do not correlate with either efficacy or safety, but if you do measure peak vancomycin levels, the Tmax is approx. 1-2 hours post infusion. Peak levels of > 35 mg/L should prompt dose adjustment.

However, dose adjustments are based on trough values which should be obtained after the 3rd dose and not exceed 15 mg/L [4].

After all this math, the surgical procedure is already well underway and it is time to call in your second antibiotic dose from the pharmacy (where a helpful colleague will have done all the necessary calculations for you). Next time you see your hospital pharmacist, thank him for doing the math for you. Obviously, he has all the modern dosing tools at his fingertips (Fig. 3).
Indeed, there are many excellent detailed dosing tools [5] and PK calculators available on the web. No need to go back to the package insert and wreck your brain.
The reader interested in the history of aminoglycoside dosing will find the recent article by Pai et al. informative [6].
References:
[1] W Goede Hosp Pharm. 2013; 48: 560
[2] http://www.cumc.columbia.edu/dept/id/documents/Clinical%20References/Aminoglycoside_Conventional_Dosing_and_Monitoring_in_Adults_ONEPAGE.pdf
[3] http://www.cumc.columbia.edu/dept/id/documents/Clinical%20References/Aminoglycoside_Conventional_Dosing_and_Monitoring_in_Adults_ONEPAGE.pdf
[4] http://www.cumc.columbia.edu/dept/id/downloads/Vancomycin_5-26-05.pdf
[5] http://www.hopkinsmedicine.org/amp/guidelines/Antibiotic_guidelines.pdf
[6] M Pai Diagnostic Microbiol Infectious Dis 78 (2014): 178
