

This is a somewhat nostalgic retro blog.
I was leafing through a book by Vince Andriole called ‘The Quinolones’.[1] First released in 1988, its third edition is from 2000. It provided in-depth coverage of quinolone chemistry, PK, microbiology, efficacy and safety. It was a great review of the large and growing field of gyrase/topoisomerase inhibitors, with chapters written by the doyens of the day. From today’s perspective, however, what we find most striking is the immense number of candidate drugs in development.
In presentations and slides Andriole reviewed more than 40 compounds at various stages of development. Of course, we still have ofloxacin/levofloxacin, ciprofloxacin and moxifloxacin on the formulary. These, drugs from JNJ and Bayer, became blockbusters at a time when blockbusters were still rare.
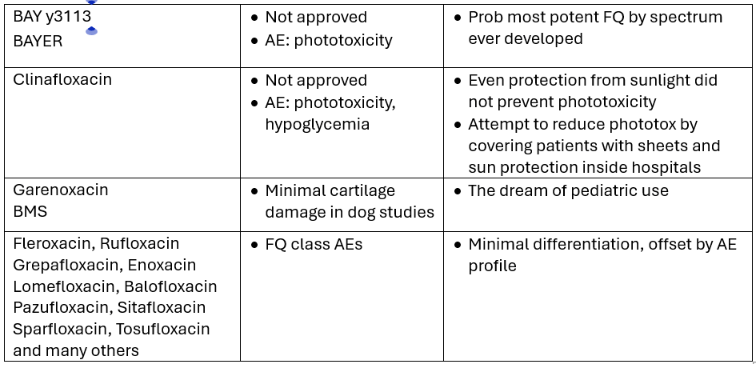
All but forgotten is the effort that went into – well, all the others! Below an admittedly incomplete list that is meant to bring back those exciting times, highlighting some key events and insights:
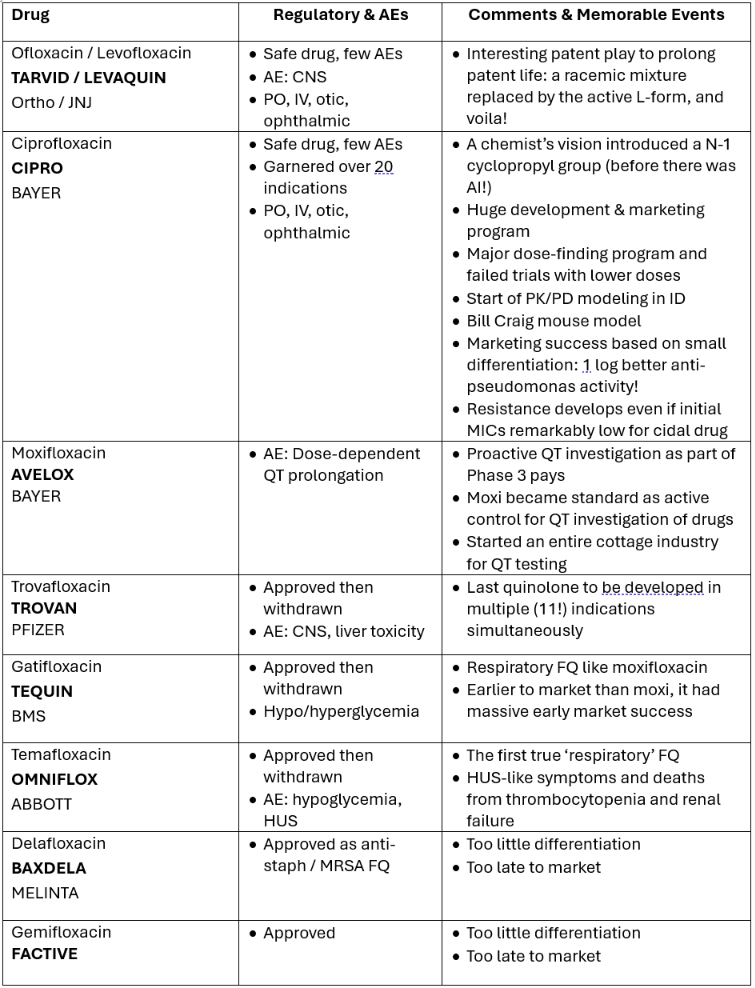
Over time, the FQ-related class AEs became clearer; they were mainly related to
- GI and hepatic side effects
- Inactivation by divalent ions with PO dosing
- QT-prolongation
- Phototoxicity
- Chondrotoxicity and tendon rupture
Many quinolones died because of the toxicities listed above. While QT prolongation was avoidable, other toxicities were not. Efficacy was always a given but safety issues often turned up only late in development.
We are still not sure why temafloxacin was associated with HUS. Young patients with trivial infections but who were otherwise healthy died if the early symptoms were not recognized. This was not a class effect, never seen in any other FQ to the best of our knowledge. However, it served as a wake-up call that even if a class of drugs is well understood, every new member warrants individual scrutiny and careful monitoring.
These toxicities represented a mine field; eventually we had an entire cemetery of FQs somewhere out there in pharma land.
Nonetheless, every Big Pharma had at least one FQ antibiotic in development. It was an attractive field for industry in those days and – despite set-backs and short duration therapy – a commercial success story. Antibacterial research benefitted from the fact that efficacy was predictable, PK was testable, and the only unknown was the AE profile. Still, FQs and antibacterial R&D were a safer bet for approval than drugs in most other therapeutic areas.
So why was antibiotic development considered lucrative then but no longer today?
The short answer is that pricing for antibiotics remained behind compared to the steep rise in prices for cancer and immunology medicines. This gap became wider over time, it accelerated with the advent of costly therapies for rare disease agents, monoclonal antibodies, and medicines for chronic diseases in general. On the ID side, only HCV therapies and some HIV drugs commanded similarly high prices.
Of course, there is still an attractive niche in ID for HIV and HBV antivirals and for certain vaccines. However, it will probably take a Black Death-like epidemic to revive interest in antibacterials, before Big Pharma sees opportunities and gets seriously involved again.
Don’t blame pharma companies for this state of affairs; they are doing exactly what’s good for them and best for shareholders. Their mandate is to maximize profits first and foremost. There is no law that demands operating altruistically.
Regulators shape the market which ultimately determines which therapeutic areas are in demand. Companies are smart enough to find areas of lucrative engagement for their risky investments. The cost of developing a novel agent is certainly over 1 billion dollars nowadays, something often ignored by those who only look at manufacturing costs for any given product.
A recent Nature article provides some insights into development costs and revenue streams for drugs approved between 2011 – 2020.[2]
The authors explain why blockbusters are needed to compensate for ‘duds’, the many drugs that fail to make it to the market. They identified a total of 36 blockbuster drugs overall, 11 in oncology and 8 in ID. All the ID blockbuster drugs are HCV, HIV, or Covid antivirals (see Table), no antibacterial or antifungal made the list.
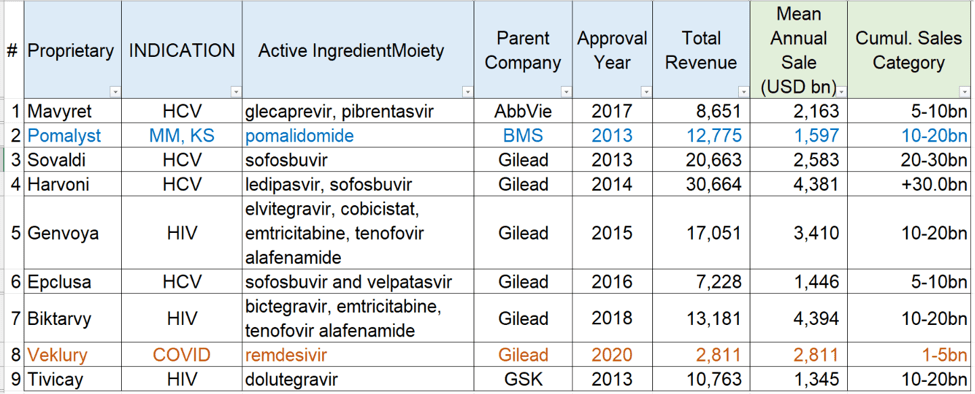
Not surprisingly, the main breakthrough occurred in the field of HCV therapeutics; these new agents truly revolutionized therapy in the past decade. Pomalyst should not be on this list; it is not an antibiotic but an immunology drug. Remdesivir flamed out early and is now almost obsolete. We reviewed the remdesivir story in a blog earlier this year [Obeldesivir].
It seems awfully high but
$2.6 billion is the estimated average total capitalized R&D cost
for the development of just 1 new drug. [2]
The economics of antibiotic development has been critically reviewed by knowledgeable and independent experts.[3] They all make the point that curative short-term antibiotics are a poor investment financially.
At least for now!
If any of this is surprising to you, you haven’t been paying attention. Welcome to the world of Big Pharma and its profit-driven philosophy! None of this is really new; frankly, it all makes good (business) sense. If society dislikes the status quo, it has the power to change the playing field and make antibacterial R&D more attractive similar to what we had in the 90s.
Some changes are sure to come; they will be made once a cry for change becomes louder because of an unforeseen epidemic. Once we reach that point, resistance is pointless. And ID folks know a lot about resistance!
ABBREVIATIONS
AE adverse event
HUS hemolytic-uremic syndrome
FQ fluoroquinolone
PK pharmacokinetics
REFERENCES
[1] Andriole, V. (Ed). The Quinolones. Academic Press, San Diego – 1988
[2] Schuhmacher A. The significance of blockbusters in the pharmaceutical industry. Nature Rev Drug Discovery 22:177, 2023
[3] Mossiakos E. Policies and incentives for promoting innovation in antibiotic research. LSE 2010
